3. IN THE WAKE OF KNOWLEDGE
3.6. Milestones in BCG work
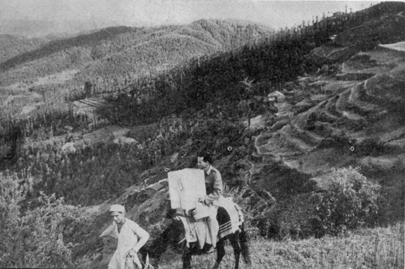
From 1951 onwards, India was covered by the BCG Mass Campaign. Approximately 170 (more than 190 at times) full-fledged teams, toured the country setting up BCG vaccination centres in both rural and urban parts, offering BCG vaccination to all. It was the first organised effort outside Europe and was the biggest campaign undertaken by any country in medical history. Even though jeeps were provided, it was to the credit of the teams that they set up camps in so many inaccessible places. India’s vast network of rural areas had no pliable roads. Sometimes, even bigger towns could be reached with great difficulty. Infrastructure like lodges and hostels was inadequate.
|
Dr. Kul Bhushan |
Dr. Pyarelal, Medical Officer |

Added to these difficulties was the cumbersome two step procedure of the vaccination itself: every one had to receive a pre-vaccination tuberculin test with 5TU PPD RT22 batch of the tuberculin, come back for tuberculin reaction measurement three to four days later and if her/his reaction was less than 8 mm in size, she/he would become eligible to receive BCG vaccination. The teams tuberculin tested 165 million and vaccinated 65 million56. In 1964, as Dr Kul Bhushan recalls in “My experiences of Mass BCG Vaccination “…..Combined efforts of the teams...helped the campaign ... . I saw dedicated workers busy for 18 hours a day... .I have known one who slept 16 hours a day and divided the remaining eight hours, judiciously into bits of two hours each between dressing, getting ready for the day’s work, sipping tea, meeting friends and taking well earned rest and food! I cannot forget the technician whose woolen suits served as a mobile refrigerator for the vaccine... . Those who walked 8-10 miles a day to cover houses in hilly areas testing small two digit figures... . It was a pleasure to see systematic coverage of areas in some states... . In a few others...it was not so...I was disappointed to see teams leaving vast areas uncovered.... I realised how easy it is to convince the public but not administrators”57...
|
|
Besides conferring the benefits of BCG vaccination, the campaign produced a wealth of data on the tuberculin sensitivity patterns prevalent in the country and indicated the hitherto unsuspected extent of the TB burden. There was an additional benefit as pointed out by Dr Benjamin. Besides making BCG available to anyone residing anywhere in the country either urban or rural, it also served as the biggest ever health education programme undertaken anywhere in the world. The masses of India became aware that the utilities provided by the Department of Health that could be used by them gratis56.
However, an assessment of the campaign’s methodology had to be made because of three major reasons. First, the teams had no option but to set up vaccination centres in some central place. Despite announcements and propaganda for people to avail of the facility, it was obvious that only action takers came to the centre. That left a large proportion of people uncovered. Second, the screening tuberculin test proved to be a deterrent. Because of fear of two pricks, absenteeism increased. It is not strange for people to question receiving two pricks for the same disease that they are not suffering from. The third was a technical one. Evidence from the earlier campaigns indicated that a majority of people over 20 years of age were tuberculin positive and therefore, ineligible for vaccination. About 97% of children (0-9 years) were tuberculin negative. The teams, therefore, were burdened with a lot of redundant work. It would be beneficial to restrict BCG to 0-19 years58.
|
Mr. Vijay Singh, |
BCG given by Multi Purpose Workers (MPWs) at Health Centres |
|
A milestone in Campaign's History VI All India BCG
Workers Conference at Bangalore |
|


The NTI studied these problem areas systematically. The 6th All India BCG Workers’ Conference was held on January 13th and 14th, 1962, at the NTI premises. Over 100 delegates from various states attended. Doctors D’Silva (UNICEF) and RH Bland (WHO) also attended and represented their organisations. Dr PV Benjamin presided. Among others, Drs GVJ Baily and Kul Bhushan of NTI presented papers. Based on the NTI studies on door-to-door BCG vaccination, Dr Baily pointed out that the coverage of vaccination improved (up to 8%) by adopting house-to-house vaccination strategy. However, the procedure was slow and the output of work would be low due to time taken up in registration of every individual of the household. Instead the team visits could be utilised as part of the DTP (such as assisting in diagnosing TB cases)56. Presenting his paper on freeze-dried BCG vaccine produced at Guindy Laboratory in Madras, Dr Kul Bhushan stated that though liquid vaccine produced slightly higher allergy than the freeze-dried vaccine, the level achieved by the latter was quite adequate. Further studies would be undertaken to assess the qualities of the Madras vaccine, as it was new59.
This led the GOI to create a DTC in each of the 318 districts. Based on the recommendations given by the conference, the GOI suggested integration of the BCG campaign with DTC. The conference was the most significant held so far. Firstly, because of the discussion regarding integration of the campaign with the GHS. Secondly, because of the presence of administrative MOs. Thirdly, because decision was taken to introduce house to house vaccination campaign during the Third Five Year Plan. Ultimately, in 1978 the BCG campaign was integrated with GHS and became part of Universal Immunization Programme (UIP).
n 1964, Gothi found that BCG vaccination could be given directly without tuberculin test. There were not many large or untoward reactions to BCG60. In 1965, Dr Kul Bhushan suggested that direct vaccination in 0-20 year age group could be carried out because it was the most vulnerable61. There were added advantages gained over the mass campaign method in terms of systematic coverage and proper record keeping. In accordance with these findings and studies, a manual for BCG workers was prepared and field tested. By 1966, 44 of the 189 BCG teams were integrated with the DTCs and gave satisfactory outputs.
However, another issue arose. Would there be any immunological interferences especially among children below one year, because they would be receiving both BCG and smallpox vaccinations? Dr Kul Bhushan found no evidence of immunological interference between the two vaccines even when administered simultaneously. Surprisingly, the acceptability of the simultaneous procedure was higher than when BCG was given alone61. By the time this scheme could be fully implemented the smallpox vaccination was discontinued, as it got eradicated in 1975.
In 1973, Baily literally wound up the mass campaign approach by making the PHC personnel like Auxiliary Nurse Midwives (ANMs) and Basic Health Workers (BHWs) responsible. They would give BCG to new borns in their areas by vaccinating them once a month in nearby sub-centres. This had great operational advantages besides reducing vaccine wastage62.
Another problem emerged following the introduction of direct BCG vaccination. As the coverage of BCG vaccination increased in the population, tuberculin surveys would be progressively rendered difficult. One may not obtain sufficient number of unvaccinated persons to represent the population to carry out tuberculin surveys for assessing the prevalence of infection. Are there ways in which information of prevalence of infection could be elicited from BCG vaccinated persons? For e.g., could BCG vaccination induration size be used as an indicator of infection with M.tb? In 1974, Gothi and others presented a paper showing that vaccination induration could be used as an indicator of tuberculous infection. Vaccination induration of 14 mm or more on fifth or sixth day appeared to be the best criterion for demarcating the infected from the non-infected. Even though there were other choices, e.g., 12 mm or 14 mm on second day etc., the choice of 14 mm on fifth or sixth day of vaccination satisfactorily demarcated persons infected with M.tb from those non-infected63.
Under Dr Kul Bhushan, the All India BCG Assessment Team was instituted for assessment work of the mass BCG teams in different parts of the country. The team was small and had to tour extensively in the most adverse conditions. During the days of the steam engine, it would take three days for the team to reach a city or town in Rajasthan from Bangalore. From there, the team had to reach its destination on whatever transport provided by the state government. It had the additional task of retesting groups of population vaccinated with two BCG vaccine strains: the Madras freeze dried vaccine and the Japan freeze dried (glutamate) vaccine. For the BCG vaccine laboratory, Guindy, it had to carry out a comparison of stock solutions of RT22 and 23 batches of tuberculins. It is to the credit of this small team that it conducted the two studies among 5-16 year old school children in West Bengal. The study was inconclusive but indicated that the increase in the storage temperature resulted in the higher loss of potency of the vaccines59. In addition, Dr Raj Narain and others had also taken up the task of comparing the allergy producing capacity of the Madras and Danish BCG vaccines. They found that the allergy producing capacity of both the vaccines was not different64.