2. THE FORMATIVE YEARS
2.3 Work done during the period
2.3.1. The Kirangur experiments
Research activities and work methodologies had to be field tested first in pilot projects. For this purpose Kirangur, a village about 125 kms away from the Institute, was selected. It is a small roadside village; hence, it was possible to take the fragile IGE X-ray unit mounted on a bus to its doorstep. Moreover, there was a conveniently located school building which could be used to set up the examination centre where doctors and technicians could work.
A study of Annexure II would reveal that nearly all the forty protocols approved by the TCC during this period had high priority in training of personnel. Both the field and the headquarters staff were being trained in carrying out different aspects of operations research.
One of the first research protocols (RP) was a pilot protocol for the training of newly recruited NTI staff, 21 BCG technicians and three senior health inspectors deputed from the Mysore state (now called the Karnataka state). They were to be trained selectively in activities like: identifying village boundaries; establishing rapport with villagers and relevant VIPs; assigning tasks to different workers and supervision of different activities; maintenance of standard of work and time schedule. At the headquarters, the supportive staff were trained in: processing of incoming data; reading of MMR films; processing sputum for microscopy, culture and other tests; data entry; analysis; preparation of summary reports and when decided upon, consolidating the information into a paper for publication.
To gain work experience in conducting major research studies several pilot studies were launched in Kirangur, Srirangapatna taluk (population:1800 in 1959-60)29,35. These were epidemiological and sociological in nature (i) A core group got experience in rapport building, contacted VIPs, selected a suitable place as examination centre etc; (ii) some prepared a location map of houses, registered residents on individual cards; (iii) others briefed and motivated the registered population and escorted them to the examination centre with identity slips; (iv) trained persons did tuberculin testing in accordance with a precoded design on a selective basis; (v) the trained vaccinator gave BCG vaccination (in different doses given selectively by design); (vi) the XT took 70 mm chest X-rays of those five years and above; (vii) symptom elicitation and clinical examination was done by a MO. A follow up team which consisted of tuberculin and vaccination scar readers, LTs and HVs, carried out: three-month and one year follow-ups.
|
Dr. VB Naidu |
|
|
1. Village field activity |
2. Village field activity |


The entire staff of NTI was shifted to the Kirangur camp. The daily work schedule at the field was between 7.00 to 11.00 a.m. and 4.00 to 7.00 p.m. Incidentally, Srirangapatna was a small town and did not have a hotel facility to provide food for this large team. Cooks were recruited and posted so that the staff could run a mess. As the town did not have a petrol bunk, a vehicle with jerry cans was sent to fetch petrol from Mysore where the nearest petrol bunk was situated. Another vehicle called the communication vehicle plied between the camp and headquarters. This carried completed forms, sputum specimens, exposed X-ray films and other materials to the NTI and brought back new forms, X-ray results, sputum results and material needed for work.
During the time field work was in progress, Kirangur village was a beehive of activity. It was a sight to see the MOs and other investigators walking up and down the dusty lanes of the village either motivating the local people to go to the examination centre or in deep consultation among themselves, sorting out technical problems. Every aspect of work was observed in detail with an eye for improvisation, unambiguous data elicitation and getting maximum coverage with minimum inconvenience to the villagers. There were discussion sessions both at the camp and at the NTI so that the work progressed as planned.
|
|
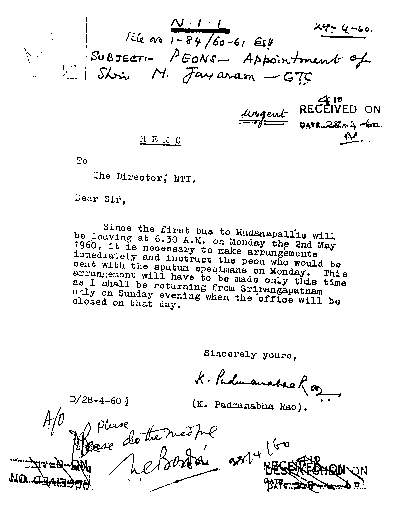
The NTI laboratory was not yet functional. Sputum specimens were arranged to be processed at UMTS, Madanapalle. The assistance rendered by the UMTS went beyond processing of sputum specimens for culture and sensitivity for M.tb. It trained two LTs of NTI on all aspects of work. The specimens brought from Kirangur by the communication vehicle had to be transported without delay. Hence, a rider on a motorcycle was retained at the NTI to immediately transfer the sputum specimen to another sputum box with sufficient ice, and transport it to UMTS. From there he would bring back sterilised empty containers and sputum results. These were processed and relevant feed-back was sent to the camp for further work. This seemingly simple task of transporting sputum specimens was not easy. If the motorcycle broke down, it was not possible to get it repaired on the same day and a stand-by was not readily available. Speedy actions were taken to send the specimens by bus and to get the motorcycle repaired. Appended photocopy shows how the speedy actions were taken in one such instance.
All senior officers, including the Director, visited the field station to benefit from practical experience so that work became accurate and less tedious, data entry forms less cumbersome and more informative. As administrators, they had to resolve practical problems like funds, fault repair, supplies and technical problems that cropped up in the field. They also worried about sudden distress calls, e.g., X-ray breakdown needing immediate attention. A different type of concern confronted the field work organisers. For e.g. Where to set up camp? Who are the village VIPs to be contacted to maximise rapport? What is the most convenient time to get maximum coverage? How to get the cooperation of the stubborn, the non-cooperative or the panicky? What strategies to adopt? These were very relevant and important factors in field work because every area, every individual, is different.
|
|

Kirangur was the first training ground for social workers to get experience in interviewing techniques. One of the Kirangur experiments was: “to examine the frequency of complications after vaccination with BCG in relation to the pre-vaccination tuberculin sensitivity”. The other minor objectives were learning census taking, tuberculin testing, reading, X-ray examination, sputum examination, by experience . Thus, these studies served the purpose of gaining experience in all aspects of field work which would be useful for future epidemiological studies as well as sociological and BCG trials, to be conducted. For the proposed major BCG Trial, the four taluks of Bangalore district, viz., Nelamangala, Magadi, Channapattana and Devanahalli, were selected. Much work was being done at NTI on planning the trial. Therefore, several experiments on BCG had been included in the work29. The proposal was ultimately shelved because of the overriding priority to conduct operations research on various aspects of the District Tuberculosis Programme (DTP). Fortunately, five years later, the BCG trial proposals were revived under the aegis of ICMR. However, the venue of the trial became Chingleput, Tamil Nadu and not Bangalore. The details of BCG trial appear in Chapter III. Thus, the Kirangur camp served the purpose for which it was established.