7.3 WEST ZONE
Study population
A total of 55,366 children were registered in the rural and urban areas of six selected districts in the zone. Of these, 51932 were subjected to tuberculin testing. While tests were performed satisfactorily among 51733 children, these were unsatisfactory among 199 (0.4%) children. Among satisfactorily tested children, 48283 were test read. Of these 22259 were without BCG scar, 25114 with BCG scar and the BCG scar status was doubtful among 910 children (Flow chart).
The proportion of children with BCG scar among satisfactorily test read children was 52%. It was about 47.4% in rural and 62.4% in urban areas. This difference was statistically significant. The proportion of children with BCG scar in rural and urban areas of individual districts is presented at table 7.3.1. The proportion of children with BCG scar in urban areas was found to be higher than in rural areas for all the districts. It was higher among males compared to females in both rural and urban areas.
The analysis for estimating prevalence of infection and ARTI was performed among 22,259 satisfactorily test read children without BCG scar.
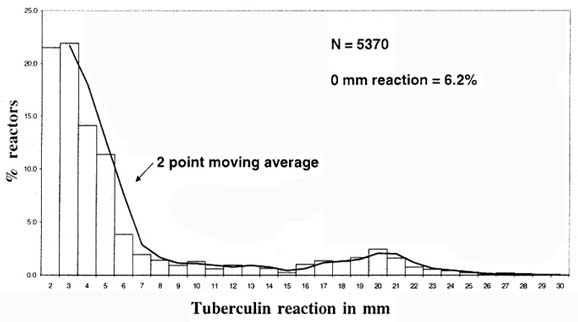
The frequency distribution of tuberculin reaction size
The frequency distributions of tuberculin reaction size among children without BCG scar in the zone and separately for rural and urban strata are presented in figures 7.3.1 to 7.3.3. It was observed to be bimodal with the mode of reactions attributable to infection with tubercle bacilli at 20 mm. There was a suggestion of an anti-mode at 15 mm.
Estimated prevalence of infection and ARTI
The prevalence of infection was estimated by the antimode as well as the mode methods adopting the following criteria:-i) Using a cut off point of 15 mm - all reactions > 15 mm in both strata were considered due to infection with tubercle bacilli (Method I).
ii) By mirror image technique considering the mode at 20 mm (Method II).
The prevalence of infection in the zone was estimated at 9.3% by antimode method and 8.5% by mirror image technique. The ARTI computed was 1.8% and 1.6% by method I and II respectively. The confidence limits are given at table 7.3.2.
A significantly higher proportion of children was found to be infected in urban compared to rural stratum, by both methods. Consequently, the estimated ARTI was higher in urban stratum than in rural. In rural stratum, the estimated ARTI was 1.5% by Method I and 1.4% by Method II. In urban stratum, the estimated ARTI was 2.4% by Method I and 2.1% by Method II.
The proportion of infected children and the estimated ARTI was found to be similar among boys and girls (P>0.05).
The ARTI when computed from the estimated prevalence for 5-9 year age group was somewhat higher than that for 1-4 year age group.
The proportion of infected children in the rural and urban areas of different districts, by method I is given in section 7.6
The proportion of children presenting with additional features viz. vesicles and bullae was 1.2%..
FlowChart
Study Population - West Zone

Table 7.3.1 : Proportion (%) of children (satisfactorily test read)
with BCG scar by District
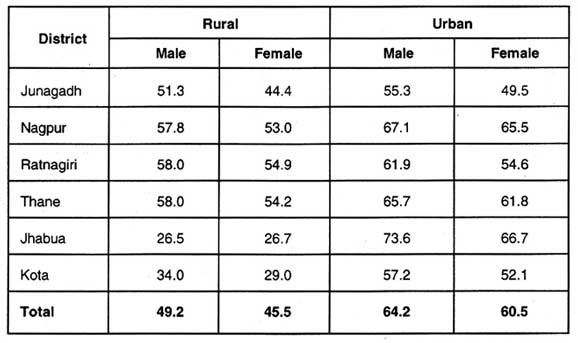
Table 7.3.2 : Prevalence of infection among children 1-9 years of age
andcomputedARTI- West zone
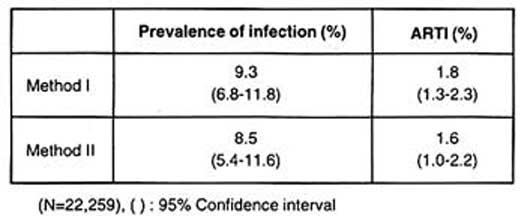
Table 7.3.3 : Prevalence of Infection and ARTI
by stratum, sex and age group
- West zone
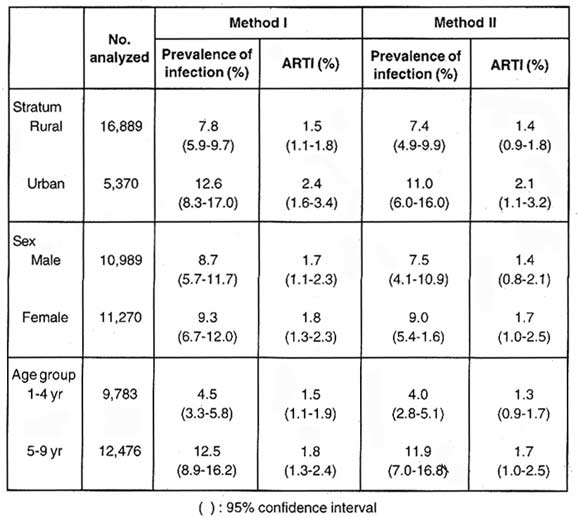
Fig. 7.3.1 : Frequency distribution of tuberculin
reaction size among
children 1-9 years of age, without BCG scar -West zone
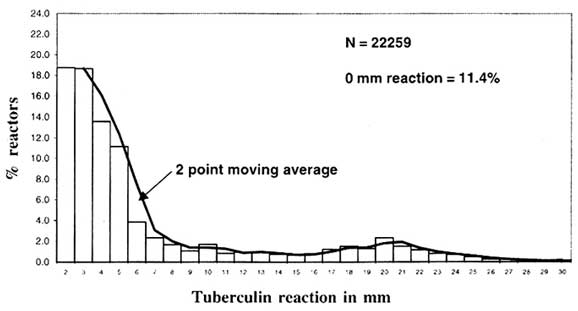
Fig. 7.3.2 :Frequencydistribution of tuberculin
reaction sizeamong
children 1-9 years of age, withoutBCGscar - rural stratum, West zone
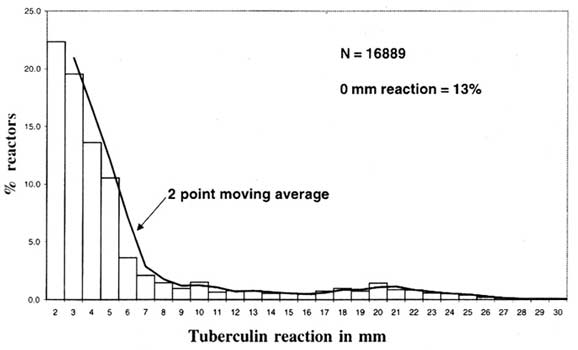
Fig. 7.3.3 :Frequencydistribution of tuberculin
reaction sizeamong
children 1-9 years of age, withoutBCGscar - urban stratum,West zone